Digital Mental Health
Designing effective digital tools for mental health.
Digital mental health interventions — from mobile apps to messaging-based therapy platforms — have grown rapidly as a means of expanding access to care. But access alone doesn't determine whether an intervention helps: many commercially available mental health apps fail to meet evidence-based principles, engagement in digital therapy remains persistently low, and the translation of evidence-based interventions into digital formats introduces design challenges that are not yet well understood. This line of research examines what makes digital mental health interventions work in people's everyday lives, and how to design them better.
This work connects closely to our research on human-centered design methods and frameworks for mental health, which addresses how to adapt non-digital evidence-based interventions and how HCI and implementation science can work together more effectively.
Models and Frameworks for Digital Mental Health
HCI's Role in Mental Health Intervention Design
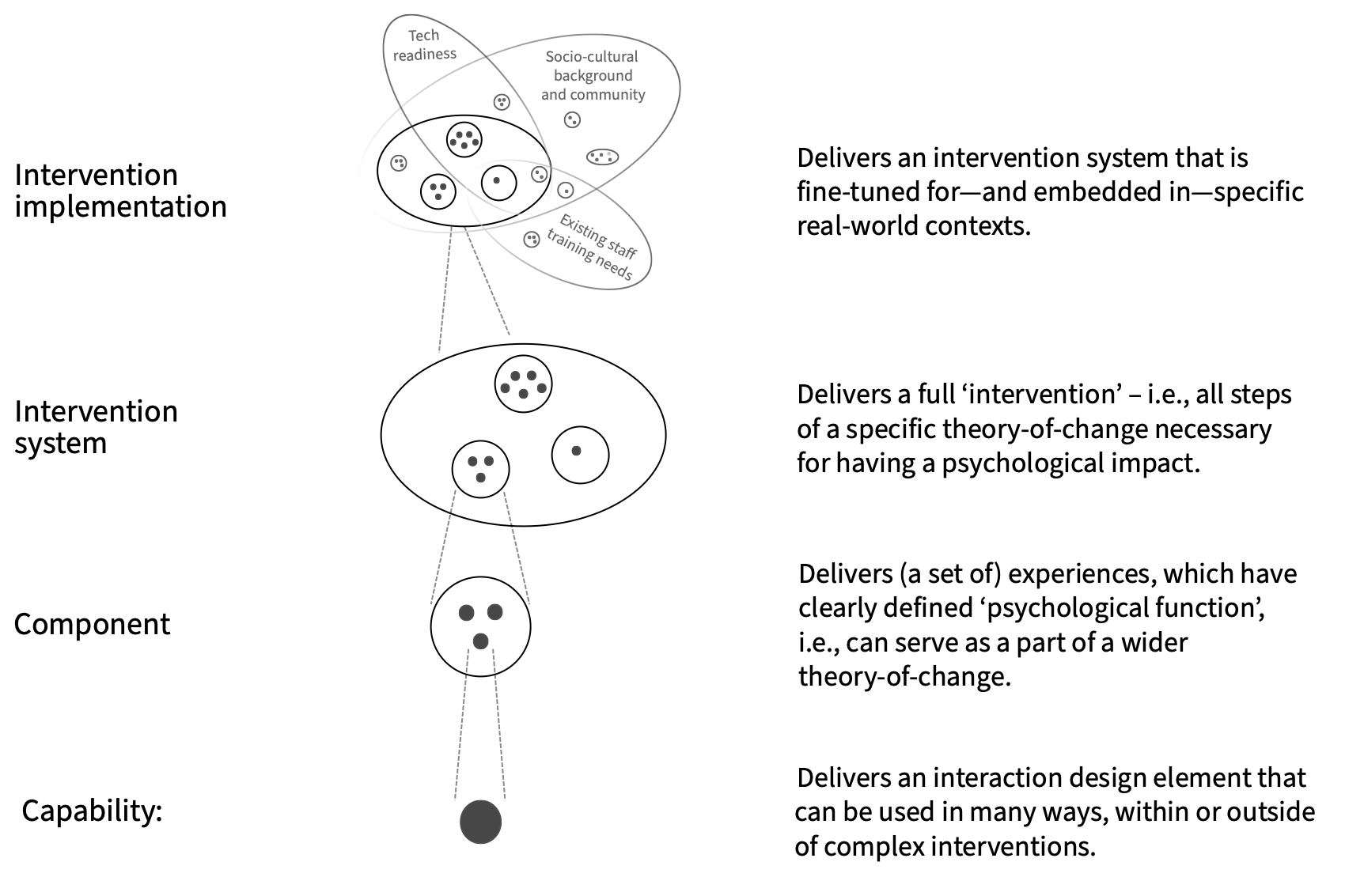
Mental health intervention research and HCI have largely developed in parallel, with limited frameworks for understanding how they can work together. Petr Slovak and I proposed a modular framework that maps HCI contributions across four stages of psychosocial intervention development — understanding the problem space, designing the intervention, evaluating it, and supporting implementation. Framed for an HCI audience, the framework helps researchers identify where their work fits within intervention development pipelines, articulate their contributions in terms that clinical and implementation science communities can use, and identify gaps where HCI has more to offer. It also provides a shared language for interdisciplinary teams building digital mental health tools.
P Slovak, SA Munson
Engagement in Digital Mental Health
Engagement is widely recognized as essential to the effectiveness of digital mental health interventions, yet the field lacks a shared model of what drives it. Across several studies, we have examined engagement from complementary angles.
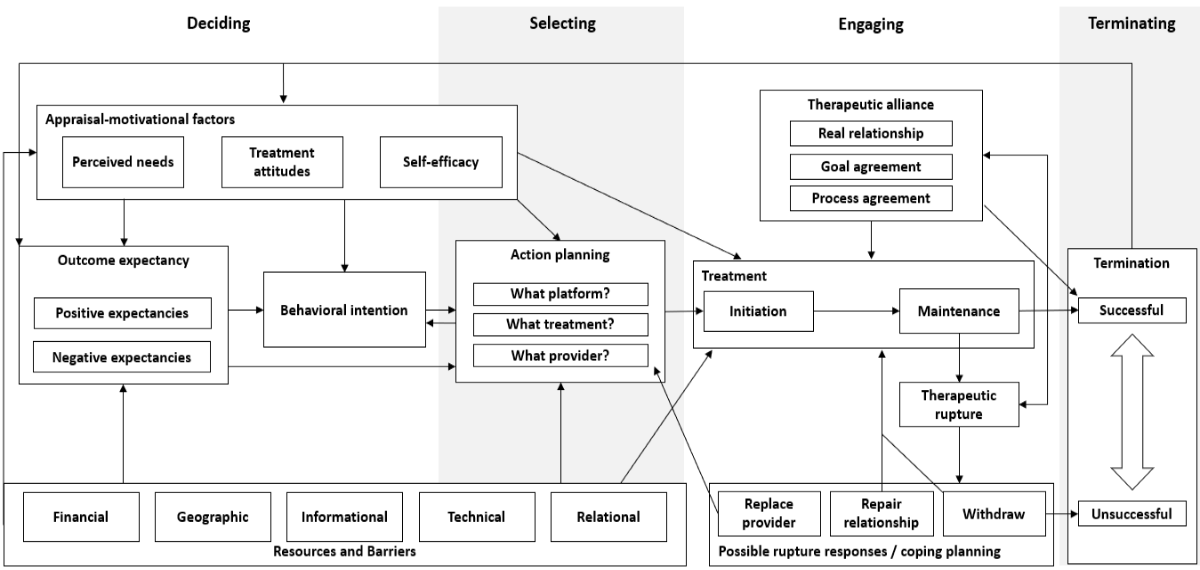
In a qualitative focus group study of users of a digital messaging therapy platform, we found that users did not see themselves as engaging with a platform so much as with a healing relationship — the therapeutic alliance with their provider was the most commonly cited factor in whether they continued or stopped treatment. We synthesized findings from this study with constructs from the Health Action Process Approach, the Lived Informatics Model, and psychotherapy process-outcome research to propose an Integrative Engagement Model of Digital Psychotherapy, covering the full arc from initial help-seeking through provider selection, treatment maintenance, therapeutic rupture, and termination.
JM Zech, M Johnson, MD Pullmann, TD Hull, T Althoff, SA Munson, N Fridling, B Litvin, J Wu, PA Arean
Goal Setting in Mental Health
Goal setting is a core component of many evidence-based mental health interventions, but the goal-setting models used in those interventions were largely designed for well-defined, short-term problems — not the complex, evolving challenges that characterize mental health. Elena Agapie led an examination of goal-setting practices in mental health contexts through a longitudinal study, finding that people's goals shift over time in ways that existing tools and intervention designs do not support well. We proposed a longitudinal goal-setting model that accounts for this complexity, offering design implications for tools that need to support people in revisiting, revising, and maintaining goals over extended periods.

E Agapie, PA Areán, G Hsieh, SA Munson
Understanding Practices & Opportunities
People managing depression assemble evolving "kits" of tools — including apps, games, and non-digital objects — most of which were not designed for mental health, yet are regularly used for that purpose. This work reorients the field from studying individual apps toward understanding the broader assemblage of tools people actually rely on, and offers design principles for building tools that complement rather than compete with what people already have.
ER Burgess, SA Munson, DC Mohr, MC Reddy
Analyzing usage data from Pocket Skills, a DBT-based mobile app, we found that skill effectiveness varied substantially across skills and user subgroups — with emotion regulation skills more effective than distress tolerance skills, in part because the latter often require activities that are infeasible in the moment. These findings point toward the importance of designing for context and toward the potential for personalized skill recommendations.
J Schroeder, J Suh, C Wilks, M Czerwinski, SA Munson, J Fogarty, T Althoff
Peer support technologies present distinct design opportunities around emotional disclosure, moderation, stigma, and community norms — and distinct challenges in balancing peer connection with clinical safety.
K O'Leary, Arpita, SA Munson, JO Wobbrock, W Pratt
Design and Evaluation
Teen Behavioral Activation (ActivaTeen)
Applying the DDBT framework, we developed and evaluated ActivaTeen, a Slack-based platform delivering behavioral activation to teenagers with depression through mood-activity logging, chatbot modules for goal-setting and barrier identification, and scaffolded peer and clinician support. Formative work used asynchronous online groups to surface teens' needs and preferences, informing the platform design. Feasibility and acceptability studies with teens and clinicians surfaced design lessons about preserving human connection, supporting peer community, and accommodating varied engagement patterns.
Arpita, C Liang, EY Zeng, K Shukla, MER Wong, SA Munson, JA Kientz
Arpita, R Nagar, J Jenness, SA Munson, JA Kientz
JL Jenness, Arpita, JA Kientz, SA Munson, R Nagar
Designing Mobile Interventions for Complex Eating Concerns
Rather than translating an existing face-to-face intervention directly into a digital format, we used a low-fidelity prototyping activity in which participants selected and implemented behavioral strategies over one week — surfacing how people make choices among treatment options, where implementation breaks down, and what support digital tools need to provide.
AK Graham, SA Munson, M Reddy, SW Neubert, EA Green, A Chang, B Spring, DC Mohr, JE Wildes